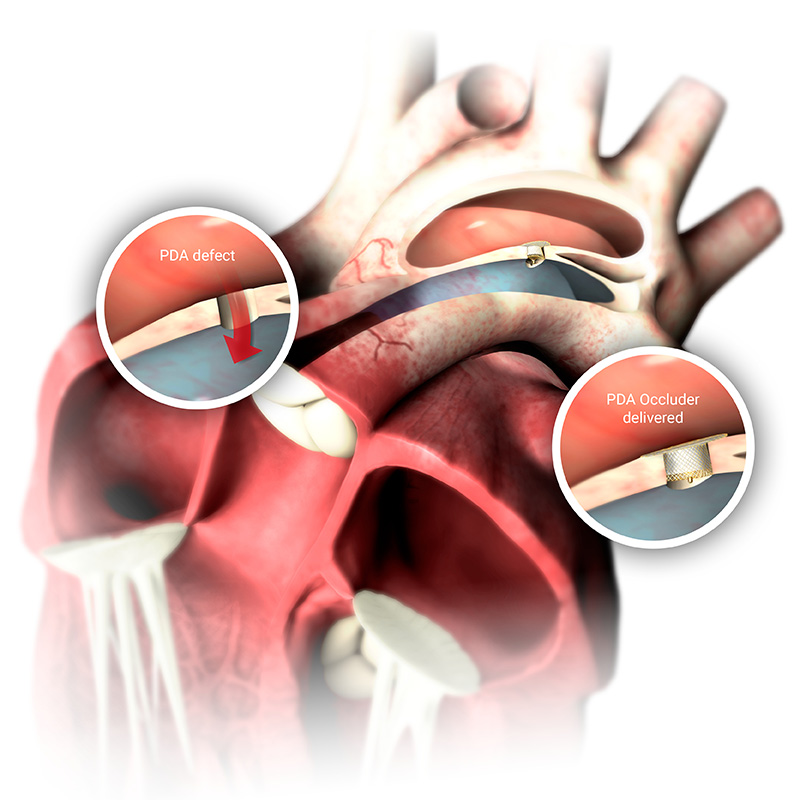
1. A heart with a patent ductus arteriosus (PDA)
2. Closing the PDA defect
3. Occlutech PDA device in position

1. A heart with a patent ductus arteriosus (PDA)
2. Closing the PDA defect
3. Occlutech PDA device in position